Results as of May 2025:
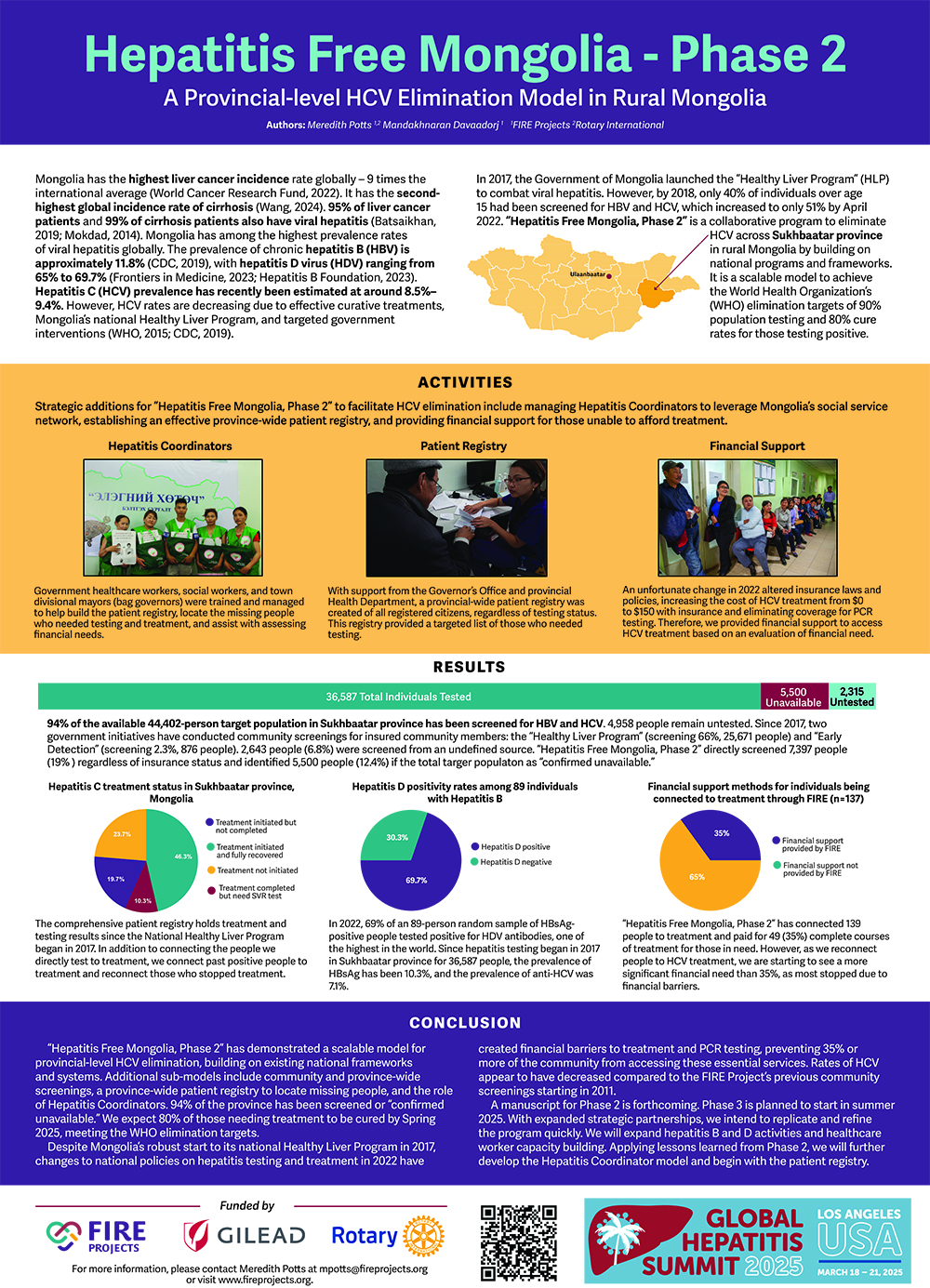
94% of the available 44,402-person population over age 15 in Sukhbaatar province has been screened for HBV and HCV. Since 2022, “Hepatitis Free Mongolia, Phase 2” directly screened 19% of the available people regardless of insurance status and identified 5,500 people (12.4%) as “confirmed unavailable. Since 2017, an additional 66% were screened by the Healthy Liver Program, 2.3% were tested by the Early Detection Program, and 6.8% were tested by an undefined program.
The World Health Organization’s (WHO) definition of elimination requires screening 90% of a community and treating 80% who test positive. 54% of the expected HCV RNA positive patients have completed treatment. 20% have started treatment. We expect 80% of those needing treatment to be cured in 2025, meeting the WHO elimination targets.
Additional Activities include:
- Conducted multiple mobile screenings reaching 14 “county (soum) clinics” 2-3 times each in 2022-2023 with comprehensive liver testing
- Directly screened 7,397 people for hepatitis B and C.
- Provided 3,535 ultrasound and 1,333 FibroScan examinations.
- Hepatologists or oncologists saw 2,516 people,
- 49 people were diagnosed with liver cancer and immediately connected to specialized care in Ulaanbaatar.
- Directly connected 137 people to treatment, paying treatment cost for 49, a financial need of 35%.
- Testing results have shown:
- 10.3% positive for HBsAg.
- 7.1% positive for HCV antibody, with 54% of those being HCV RNA positive.
- In 2022, 69.7% of 89 random HBsAg-positive samples had positive HDV antibodies.
- HBsAg positivity is 11.2 % among 25-34 year olds who were vaccinated at birth within the first 24 hours.
- Trained 150 social and healthcare workers and “bag governors” throughout the project to be Hepatitis Coordinators to leverage the government’s social service network, registration system, and patient registry.
- Managed a network of 20 lead Hepatitis Coordinators to find the missing people.
Conducted advocacy meetings with community, government and business leaders selected by the Health Department to bring the community’s logistics and financial influences together to implement further solution-based programming.
Held a community fair and distributed thousands of liver health pamphlets.
“Hepatitis Free Mongolia, Phase 2” demonstrates a scalable model for provincial-level HCV elimination, building on existing national frameworks and systems. Additional sub-models include community and province-wide screenings, a province-wide patient registry to locate missing people, and the role of Hepatitis Coordinators.
In the fall of 2017, FIRE worked with the Rotary Club of Ulaanbaatar and the Rotary Club of Flagstaff to implement “Hepatitis Free Mongolia, Phase 1,” a Rotary-funded Global Grant. “Hepatitis Free Mongolia, Phase 1” visited every county and rural public hospital in the province.
Throughout this project, 5,017 people were screened for hepatitis B and C with blood tests, FibroScan, ultrasound examinations, and physical examinations by specialists in 14 locations across Dornod province. 1,966 people were vaccinated against HBV, 36 healthcare workers were trained, 20 computers were delivered, 50,000 information pamphlets were distributed, and 20 community leaders participated in an advocacy meeting.
From the total budget, 8% was saved and redirected to training healthcare workers and social workers to be Hepatitis Coordinators in Dornod and Tov provinces in 2018 and 2019. For more information about “Hepatitis Free Mongolia, Phase 1,” please view our Phase 1 final report.



















